General Considerations
- Most often as result of degeneration of bicuspid aortic valve
- Less commonly rheumatic heart disease or secondary to degeneration of a tricuspid aortic valve in person > 65
Location
- Supravalvular
- Uncommon
- Associated with William’s Syndrome
- Hypercalcemia
- Elfin facies
- Pulmonary stenoses
- Hypoplasia of aorta
- Stenoses in
- Renal, celiac, superior mesenteric arteries
- Valvular
- Most common
- Either congenital (from a bicuspid aortic valve) or acquired
- Bicuspid aortic valve is the most common congenital cardiac anomaly
- Subvalvular
- Associated with
- Hypoplastic left heart syndrome
- Idiopathic Hypertrophic Subaortic Stenosis
- Hypertrophic cardiomyopathy
- Subaortic fibrous membrane
Types
- Congenital aortic stenosis (more common)
- Most frequent congenital heart disease associated with intra-uterine growth retardation (IUGR)
- Subvalvular (30%)
- Valvular (70%)
- Degeneration of bicuspid valve
- Supravalvular
- Acquired aortic stenosis
- Rheumatic valvulitis
- Almost invariably associated with mitral valve disease
- Fibrocalcific senile aortic stenosis
Clinical Findings
- Asymptomatic for many years
- Classical triad
- Angina
- Syncope
- Shortness of breath (heart failure)
- Systolic ejection murmur
- Carotid pulsus parvus et tardus
- Diminished aortic component of 2nd heart sound
- Sudden death in severe stenosis after exercise
- Diminished flow in coronary arteries causes ventricular dysrhythmias and fibrillation
- Decompensation leads to left ventricular dilatation and pulmonary venous congestion
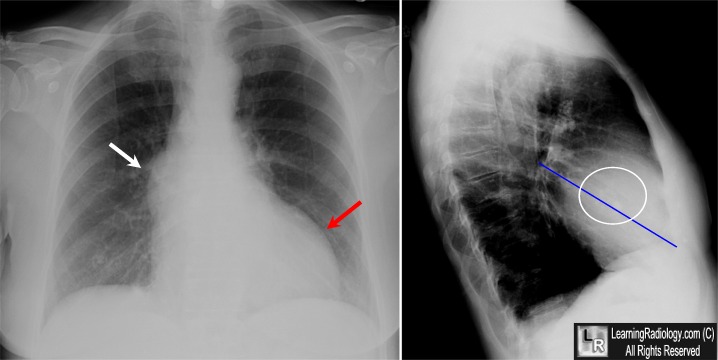
Imaging Findings
- In older children or young adults
- Prominent ascending aorta
- Poststenotic dilatation of ascending aorta
- Left ventricular heart configuration
- Normal-sized or enlarged left ventricle
- Concentric hypertrophy of left ventricle produces a relatively small left ventricular chamber with thick walls
- Heart size is frequently normal
- In adults >30 years
- Prominent ascending aorta
- Poststenotic dilatation of ascending aorta
- Calcification of aortic valve (best seen on RAO)
- In females, usually indicates hemodynamically significant aortic stenosis
- Calcification of the valve usually indicates a gradient across valve of > 50mm Hg
- Calcification begins in bicuspid and rheumatic valve in 4th decade but not until > 65 in tricuspid
- DDx
- Calcification of aortic annulus in elderly
- Calcified coronary artery ostium (thickened cusp echoes only in diastole)
- Normal to enlarged left ventricle
Echocardiographic findings
- Thickened and calcified aortic valve with multiple dense cusp echoes throughout cardiac cycle (right > non-coronary > left coronary cusp)
- Decreased separation of leaflets in systole with reduced opening orifice (13-14 mm = mild AS; 8-12 mm = moderate AS; <8 mm = severe AS)
- ± Doming in systole
- Dilated aortic root
- Increased thickness of LV wall (= concentric LV hypertrophy)
- Hyperdynamic contraction of LV (in compensated state)
- Decreased mitral EF slope (reduced LV compliance)
- LA enlargement
- Increased aortic valve gradient (Doppler)
- Decreased aortic valve area (unreliable)
Angiographic findings
- Simultaneous LV and aortic pressures recordings yield valve gradients from left heart catheterization
- Angiographic technique uses standard RAO left ventriculogram and an aortogram using a 40° LAO projection
- A non-calcified, bicuspid valve reveals thickening and doming of the valve leaflets in systole
- A jet of non-opacified blood is visible through stenotic valve
- Congenitally bicuspid valves still usually have three aortic sinuses with one large non-coronary sinus equal in size to the other two
- Calcification begins in the bicuspid and rheumatic valve in the 4th decade but not until >65 in tricuspid
- In rheumatic disease, the aortic valve commissures usually fuse whereas they do not in the degenerated tricuspid valve
Differentiating Causes of Aortic Stenosis
Etiology/Findings
|
Calcification
|
Other clues
|
Congenital Bicuspid Valve
|
30’s
|
Jet effect on aortogram
|
Degeneration of Tricuspid Valve
|
> 65
|
Coronary artery ca++
Commissures don’t fuse
|
Rheumatic dz in Tricuspid Valve
|
30’s here; teens in 3rd
world countries
|
MS or MR almost always present;
commissures fuse
|
Valve areas
Normal
|
Mild
|
Severe
|
Critical
|
2.6-3.5cm2
|
1.3-1.7
|
1.0
|
0.5
|
|
No comments:
Post a Comment