- Average age is 60-70
- Men much more common than women
- Most have an elevated serum protein with 80-90% in the globulin fraction, especially IgG
- Bence-Jones protein in 40-60% of patients (light chains)
- Osteoporosis is most common skeletal abnormality in this disease
- Lesions are usually multiple and found in vertebrae, ribs, skull, pelvis, and femur
- Over 50% of solitary lesions are found in vertebrae
- Mandible involved in 1/3 of patients with diffuse involvement
- Widespread lucencies in bone
- Discrete, “punched-out” lesions
- Uniform in size
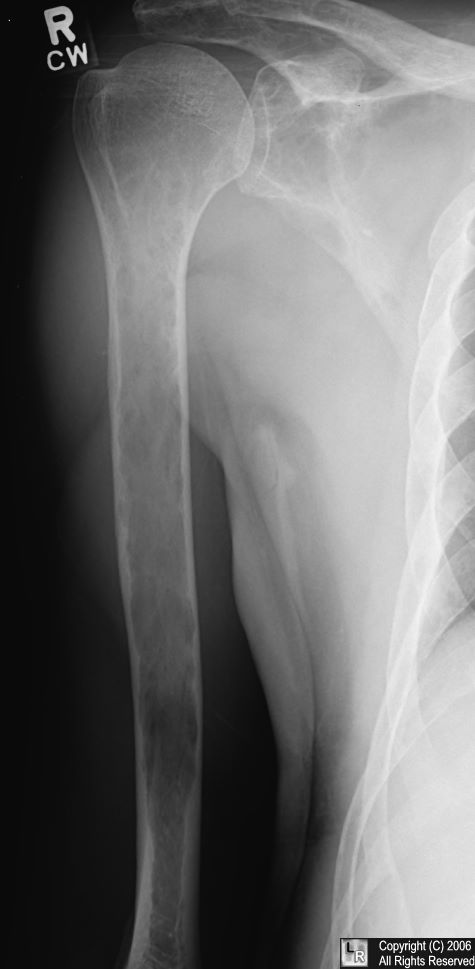
- Distinctive to MM are the lucent, elliptical, subcortical shadows, especially in long bones=endosteal scalloping
- Due to buttressing since MM is usually a slower process than mets
- In spine, MM destroys body and spares pedicle
- MM is more widespread
- More discrete holes in MM
- Large foci of coalescence more often due to mets
- Severe disuse osteoporosis may simulate bone changes of MM
- Bone scans may typically be negative and many hot areas on scan may be healing fractures
- Solitary plasmacytoma produces “soap-bubbly” expansile, septated lesion, when characteristic

Multiple myeloma . The pelvis contains numerous lytic lesions without reactive sclerosis which
have an almost "soap-bubbly" appearance in the ischia. There are also lytic lesions in
both proximal femora.
Other examples of Multiple Myeloma (Click on each to enlarge)



No comments:
Post a Comment